
Lewy Body Dementia: The Bridge Between Alzheimer’s and Parkinson’s
July 10, 2023 | Raquel Paz Bergia | Neurology
Lewy Body Dementia isn’t a medical disease that you hear about every day although it is estimated that in 2021 over 1.4 million people were affected only in the United States. The reason for the lack of public recognition is that it is commonly confused with the two most common neurological disorders, Parkinson’s and Alzheimer’s.
Lewy body dementia (LBD) is a disease associated with abnormal deposits of a protein called alpha-synuclein. These deposits are called Lewy bodies and are the clumps of abnormal protein particles that accumulate in the brain.
LBD is the umbrella for two major clinical diagnoses: Dementia with Lewy Bodies and Parkinson’s Disease Dementia.
How are these two similar, and how are they different?
The Davis Phinney Foundation defines DLB as, “a type of dementia that causes problems with memory and thinking abilities that are severe enough to interfere with everyday activities. It specifically affects a person’s ability to plan and solve problems, called executive function, and their ability to understand visual information” and defines PDD as a “dementia that develops after several or many years of living with Parkinson’s”.
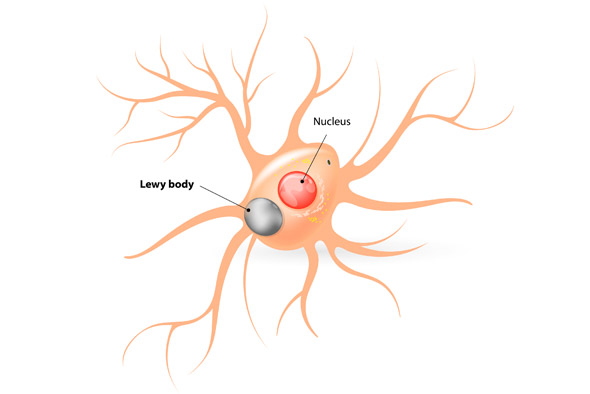
The reason why both of these are branched under LBD is that patients with either diagnosis experience the deposits of Lewy bodies into their neurons, which can be seen in the image below by ProMedica Senior Care.
So, why is it that LBD is known as the “bridge” between Alzheimer’s and Parkinson’s Disease?
LBD and Parkinson’s disease (PD) have several similarities. Both conditions involve the accumulation of Lewy bodies in the brain, which are abnormal protein deposits composed mainly of alpha-synuclein. Many individuals with LBD initially present with motor symptoms similar to those seen in Parkinson’s disease, such as tremors, rigidity, bradykinesia (slowness of movement), and postural instability. Over time, individuals with PD can develop cognitive decline and dementia, leading to the diagnosis of Parkinson’s disease dementia (PDD).
LBD also shares some characteristics with Alzheimer’s disease (AD), the most common cause of dementia. Both LBD and AD are associated with cognitive decline and memory impairment. Individuals with LBD often experience cognitive symptoms similar to those seen in AD, including memory loss, confusion, and difficulty with attention and problem-solving. Additionally, both conditions can involve changes in behavior, mood fluctuations, and visual hallucinations.
Although it shares similar traits with both AD and PD, some things distinguish it from these disorders.
LBD is characterized by a combination of cognitive and motor symptoms. In contrast, AD primarily manifests as a progressive decline in memory and cognitive function, while PD primarily presents with motor symptoms such as tremors, rigidity, and bradykinesia. LBD encompasses both cognitive symptoms, such as memory loss, confusion, and attention difficulties, as well as motor symptoms resembling those of PD.
Visual hallucinations are a prominent feature of LBD and often occur early in the course of the disease. They are less common in AD and occur relatively late in the disease progression. PD can also involve hallucinations, but they are typically less vivid and occur in the later stages.
LBD is characterized by significant fluctuations in cognitive function, alertness, and attention. These fluctuations can occur throughout the day and can lead to periods of confusion and disorientation. AD and PD do not typically exhibit the same degree of cognitive fluctuations.
Individuals with LBD may be more sensitive to certain medications, particularly antipsychotic drugs, which can worsen their motor symptoms and lead to severe side effects. This sensitivity is not as pronounced in AD or PD.
This sparks the question, how is LBD treated? Can it be cured?
Currently, there is no cure for LBD. Therefore, treatments primarily focus on managing symptoms, improving quality of life, and providing support to individuals and their caregivers.
- Medications: Certain medications can be prescribed to address cognitive symptoms, movement problems, hallucinations, and sleep disturbances associated with LBD. However, it’s important to note that medication responses can vary among individuals, and the potential benefits and risks need to be carefully evaluated by a healthcare professional.
- Supportive therapies: Physical and occupational therapy can help manage movement difficulties and maintain functional independence. Speech therapy may assist individuals with speech and swallowing difficulties. Additionally, counseling and support groups can provide emotional support and practical advice for individuals and caregivers coping with LBD.
- Environmental adaptations: Modifying the living environment can enhance safety and reduce the risk of falls and injuries. This may involve removing trip hazards, installing handrails, improving lighting, and using assistive devices to aid mobility.
- Caregiver support: Caring for someone with LBD can be demanding, so caregivers need to seek support from healthcare professionals, support groups, and respite care services. These resources can provide guidance, education, and assistance in managing the challenges associated with LBD caregiving.